No one outside of Mr. Mugabe’s inner circle, of course, can say with certainty why he has pursued policies since 2000 that have produced economic and social bedlam. For his part, Mr. Mugabe says Zimbabwe’s chaos is the product of a Western plot to reassert colonial rule, while he is simply taking steps to fight that off.
Among many outside that circle, however, the growing conviction is that Zimbabwe’s descent is neither the result of paranoia nor the product of Mr. Mugabe’s longstanding belief in Marxist economic theory. Instead, they say, Zimbabwe is fast becoming a kleptocracy, and the government’s seemingly inexplicable policies are in fact preserving and expanding it.
. . .
Mr. Mugabe’s government declares currency trading illegal, but regularly dumps vast stacks of new bills on the black market, still wrapped in plastic, to raise foreign exchange for its own needs, business leaders and economists say.
The nation’s extraordinary hyperinflation, last pegged by analysts at 10,000 percent a year, is an economic disaster that, by all accounts, the government needs to address. Yet after it ordered merchants in July to slash their prices, cadres of policemen and soldiers moved into shops to enforce the new controls, scoop up bargains and give friends and political heavyweights preferential access to cheap goods.
. . .
Mr. Mugabe’s 25-bedroom mansion in Borrowdale, the gated high-end suburb of Harare, the capital, is the locus of a boomlet that has spawned luxury homes for government and party officials. (Mr. Mugabe said his mansion was built with goods and labor donated by foreign governments.)
Mr. Mugabe arrived to open Zimbabwe’s Parliament this month in a Rolls-Royce. Equally telling, the legislature’s parking lot was crammed with luxury cars.
Such riches have been accompanied by a steep decline in living standards for just about everyone else. The death rate for Zimbabweans under the age of 5 grew by 65 percent from 1990 to 2005, even as the rate for the world’s poorest nations dropped. Average life expectancy here is among the world’s lowest, according to the United Nations.
For the full commentary, see:
(Note: ellipses added.)

 Genentech CEO Dr. Arthur D. Levinson. Source of image: online version of the WSJ article cited below.
Genentech CEO Dr. Arthur D. Levinson. Source of image: online version of the WSJ article cited below. Source of graph: online version of the WSJ article cited above.
Source of graph: online version of the WSJ article cited above.
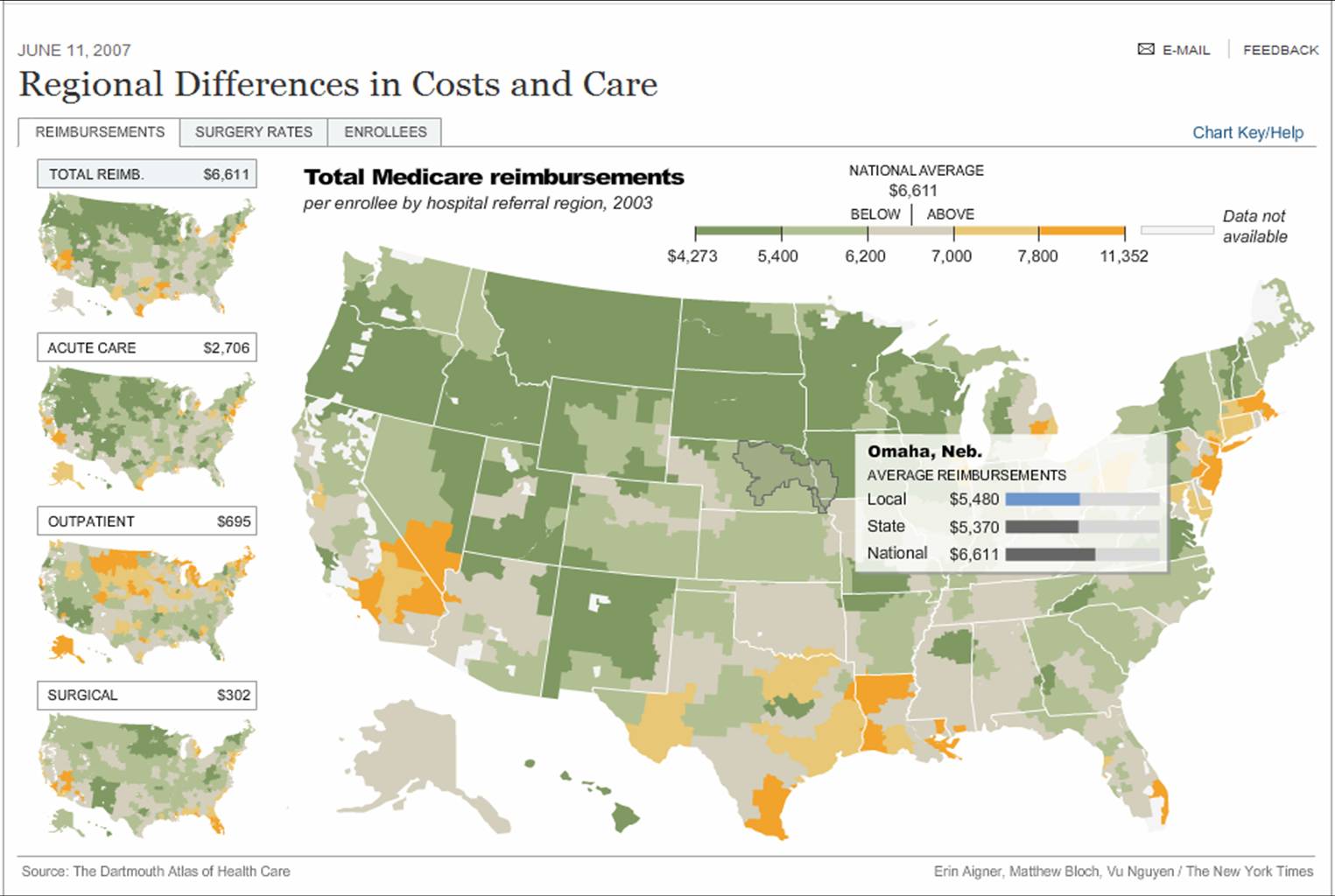
 Source of graphic: online version of the NYT article quoted and cited below.
Source of graphic: online version of the NYT article quoted and cited below.